
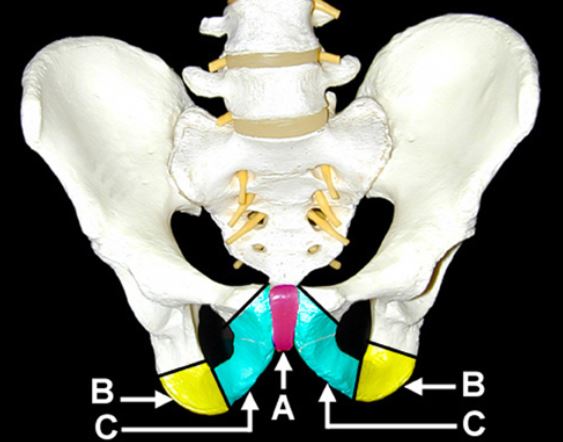
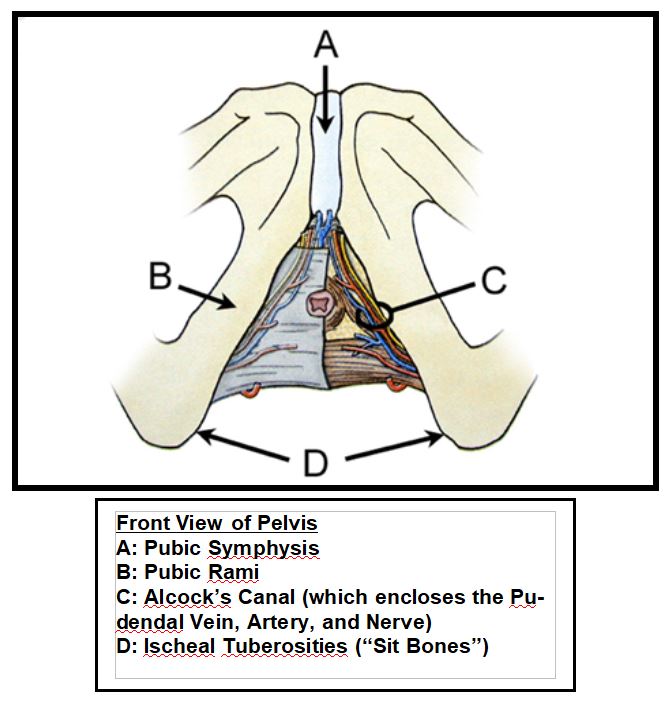
Bones of the Pelvis (front view)
A: Pubis Symphysis
B: Ischeal Tuberosities (Sit Bones)
C: Inferior portions of Pubic Rami
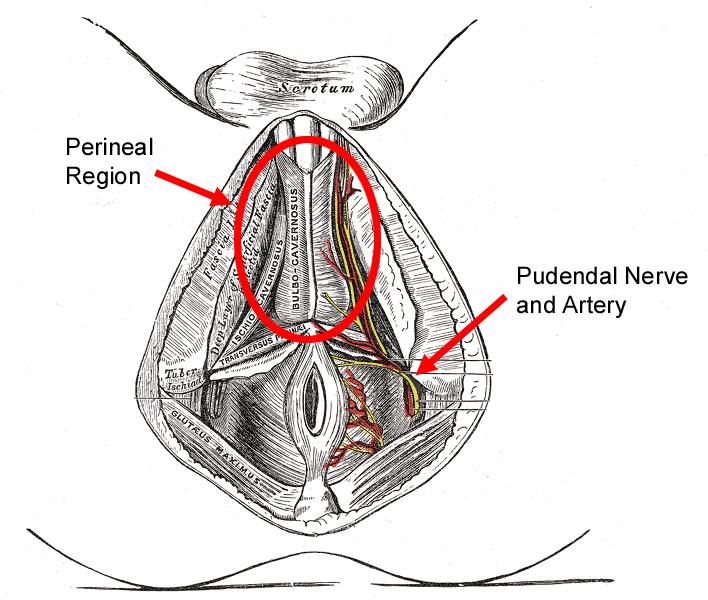
The medical dictionary defines the perineum as “the external region between the vulva [a woman’s external genitalia] and the anus in a female or between the scrotum and anus in a male.” Externally, this represents a very small region. Internally, there are plenty of complex structures that are affected by external pressure such as by a bicycle seat.
Where is the “taint”? Taint is a slang term that many cyclists use to refer to the perineum. According to Wikipedia, it is considered “lewd and mildly obscene”. Although its origins are not clear, it has no medical basis and comes from the combination of “it” and “ain’t”. It is often described as coming from the phrase, "It ain't your balls and it ain't your ass." I prefer not to use the term, and you won’t see it again in this text.
Every cyclist tends to sit on the bicycle seat in their own way due to differences in flexibility, bike fit, perception of comfort, varying amounts of muscle and fatty tissue, and riding style. Because of these factors, one seat design would have great difficulty working for every rider without some modification. However, the pelvis is pretty much the same as far as the location of arteries, nerves, and bony landmarks from person to person. The way these structures respond to stresses created by the bicycle seat is also generally the same from person to person. Therefore, if a cyclist knew where the important, sensitive structures were located in the pelvis and how they relate to the saddle contours, that person could reasonably evaluate the key elements of any seat design to decide if the seat would work well from an anatomic or ergonomic standpoint.
Female Anatomy
It is difficult to tell just how many more women are becoming active in bicycling by looking at previous studies alone. Percentages of female riders vary widely from 11% or less up to 48%, which was reported by a 2002 U.S. Department of Transportation randomized survey of over 2,500 cyclists. If the increasing numbers of women-specific products are any indicator, however, the bicycle manufacturing companies have definitely noticed this underserved and growing population of riders.
New “female-specific” product lines are popping up every day. There are women’s helmets, gloves, eyewear, cycling wear, and even full bicycles designed just for a woman’s proportions. It can sometimes be difficult to tell if these products are really made differently for women, or if they are just smaller versions of the men’s product in a different color. Bicycle seats, in particular, have initiated many discussions regarding how a woman’s seat should differ from a man’s. Two of the most significant differences between the female and male pelvis are; the placement of the external genitalia, and the differences in proportions between the male and female pelvic structures.
Many research studies that focus on blood flow to the genitals during cycling relate specifically to the male anatomy. The main reason for this is the ability to run physiological testing on males while riding on a bicycle seat without using invasive instruments or any device that would interrupt the normal interaction between the rider and the saddle. Many of the studies have used a small oxygen monitor that can be applied to the tip of the penis to monitor blood flow while cycling. This will be discussed in more detail in later chapters. Because of the tendency for many bicycle seat studies to be male-centric, many women are quick to ignore the results or assume that the results only apply to men’s seat designs. There are many reasons, however, why this may not be an accurate assumption.
Although doctors can tell the sex of a baby very early on in a pregnancy, during the development of the fetus, both the male and female genitalia originate from very similar structures.
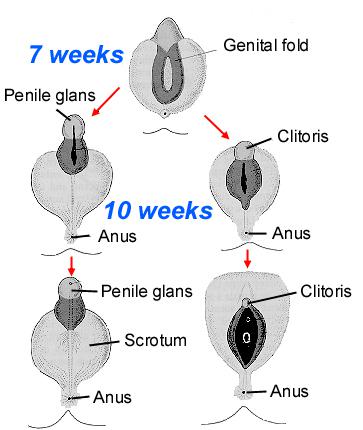
Diagram showing the analogous development of the male (left) and female (right) sexual organs during fetal development
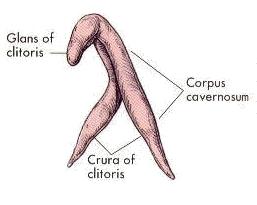
As a result of male and female genitals originating from similar structures, both sexes share analogous arteries and nerves in this region. In women, though, these arteries and nerves connect to the clitoris instead of the penis. Both the clitoris and penis are also similar in that a large portion of the organ is actually inside of the body. As you can see from the pictures below, the majority of the clitoral tissue is located along the inner borders of the pelvic bone, which is precisely the same region where traditional saddles place the most pressure while leaning forward on a seat.
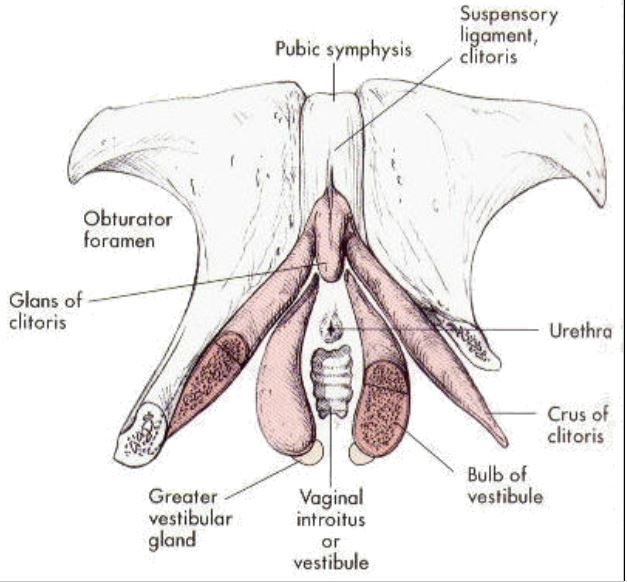
As a result of these similarities to males, women can suffer many similar conditions from using a bicycle saddle. For example, many women have reported symptoms ranging from numbness and tingling to decreased sensitivity in the genital region. The proximity of the external female genital tissues, also known as the vulva, to the seat surface can result in many painful symptoms. Problems that can occur include; labial inflammation, inflammation of the vulvar region (vulvitis), pressure/ saddle sores, and other symptoms related to chafing of sensitive genital and urinary structures.
It all adds up to a lot of discomfort while riding and not a lot of excitement after the ride. Therefore, concerns regarding the distribution of pressure over the saddle and the relation of the anatomy to the seat are equally relevant to both males and females. In effect, a bicycle seat design that avoids compression of the pudendal arteries and nerves in the male will also avoid compression of similar arteries and nerves in the female. Design considerations for the vulvar tissues would also have to be made in a saddle designed for women.
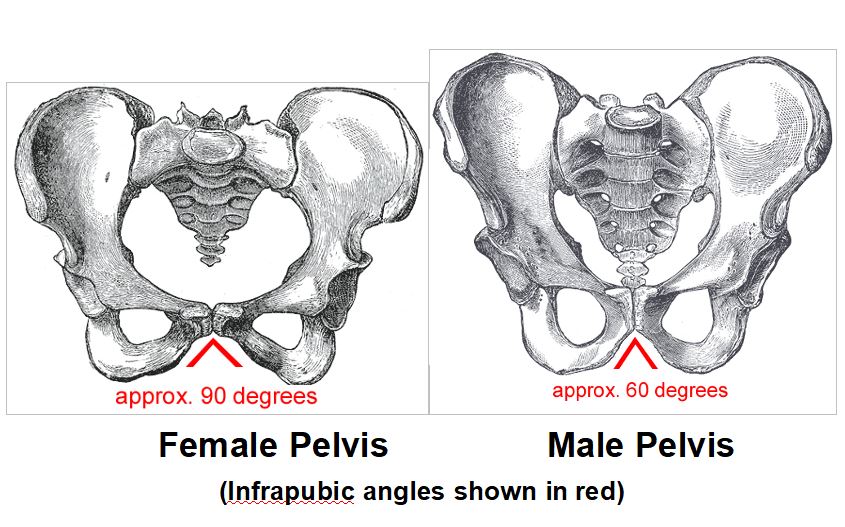
Women just need wider seats, right? Wrong. Many recent female specific bicycle seat models have focused on the increased width of the sit bones in the female pelvis. However, it is not true that all women have a greater distance between their sit bones. The actual difference between the sexes occurs at the infrapubic angle. A female’s infrapubic angle is larger by approximately 30 degrees. This results in a wider separation between the sit bones and thus a larger pelvic opening for childbirth. The actual distance between the sit bones, however, can vary significantly among individuals. The width between the sit bones is not directly related to a person’s height or stature, and shorter individuals can often have a broader pelvis. Additionally, since the overall size of any given female pelvis may be smaller than a male’s pelvis, many women with proportionally smaller pelvises may find that their sit bones can be well supported on a seat that is usually marketed towards men. As a general reference, a recent bicycle seat study at the University of Wisconsin-Madison found that the female subjects’ sit bone widths averaged 134.9mm while the men’s sit bone widths averaged 116.5mm. The measurement was taken from center to center between the sit bones. [4]
In the University of Wisconsin study, the width of the sit bones was measured by having the subjects sit on a foam block that was placed on a foot stool which was placed against the wall. The subjects were told to put their backs against the wall and slide down until they made an imprint in the foam block. Ball bearings were then placed in the indented foam to find the lowest points, between which the measurements were taken.
This technique is similar to popular methods that have been created by bicycle saddle manufacturers for use in retail stores. Both Specialized and Topeak have made boards with a deformable foam top layer used to measure the distance between sit bones.
When you sit on these devices, the store clerk should instruct you to sit in a similar position as the one used in the Wisconsin study. The purpose is to find the distance between the sit bones, which are most prominent when sitting in an upright position with your hips slightly below your knees. If you were to try to replicate your forward-bent riding position on the pad, your sit bones would roll upwards and back off of the pad. You would be left with indentations of your hamstrings and glutes, which would not leave any clear imprints and would be of little use for determining the sit bone width. The saddle widths that are recommended from these measurement pads often refer to the maximum measured width of the suggested saddle, which may or may not be flat enough at that width to actually support your sit bones.

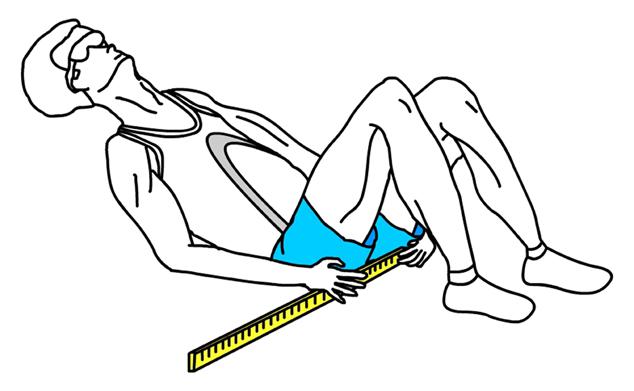
This distance can also be measured with a straight ruler. To do so, lie on your back with your knee bent. Place the end of the ruler in the approximate center of your left ischeal tuberosity and mark the distance to the approximate center of the other ischeal tuberosity with your other hand. You can usually palpate the medial and lateral borders of each sit bone, so you will have to approximate the center of each. This introduces more error, so use this only as a general reference.

Although the foam pad can tell you your sit bone width, it does not replicate actual riding posture. The pelvis of a female cyclist riding in the drops is rotated forward 24 degrees as compared to upright sitting. The Wisconsin study found that women displayed significantly greater forward tilt of the pelvis while riding in the drop handlebar position than men (~3 degrees more forward pelvic rotation). Although the authors could not explain exactly why this occurred, it significantly impacts the requirements of a saddle design. As the pelvis rotates forward, less pressure is placed through the sit bones and more weight is transferred to the pubic rami and pubic symphysis. The further forward your pelvis rotates, the less your sit bone width matters in relation to the saddle support surface since the sit bones are not the main weight bearing regions any longer.
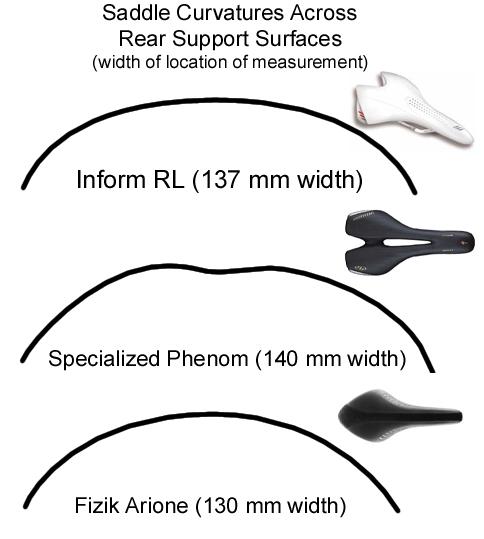
The top curvature of the saddle takes on particular importance for women’s saddle designs. When viewed from behind, a standard saddle has a convex upward curvature. The increased infrapubic angle of a woman’s pelvis makes it more likely that the seat will be able to press up into the perineal region between the pubic rami and sit bones. The University of Wisconsin study demonstrated that the increased proportional width of the female pelvis causes the centralized pressure to increase significantly as compared to the male’s pressure pattern.
Saddle designs may be able to minimize this effect by creating a flatter top surface that avoids pressing up between the bony structures. Here are some examples of the curvatures of the rear support surface of three current saddles (approximated with a deformable metal rod). Note that the Bontrager Inform RL saddle was based on the University of Wisconsin study.
Ideally, a saddle should minimize central perineal compression with a flattened central support surface and edges of the saddle that taper down gradually to allow for normal pelvic motion.
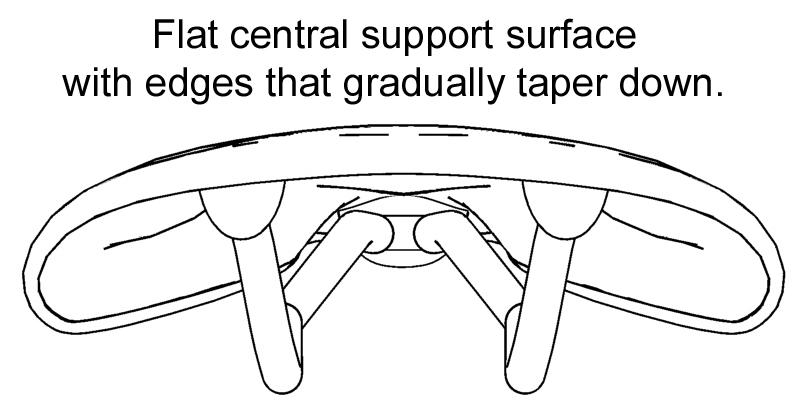
As seen in the two images below, saddles can offer dramatically different degrees of curvature through the rear support surface.

Many women often look for “female specific seats” with holes cut out through the seat for relief from the pressure created by standard racing saddles. A recent study asked twenty female cyclists to assess the comfort of three different seat designs (a seat without a nose, another with a complete hole cutout, and a standard seat design without a cutout). Fifty-five percent of the riders rated the complete cutout as the most comfortable. However, a large percentage of women (30%) rated the standard seat without a cutout more comfortable than both the nose-less and complete cutout designs. [5] This implies that a significant number of women felt that both alternative designs had no substantial comfort benefit over a standard seat design.
Although extensive statistics are not available about the incidence of cycling related injuries in females, a study from the Brugmann University Hospital reported that among a sample of 60 competitive female cyclists, one in six had complaints of lymphatic swelling in the vulvar region from the bicycle saddle. In addition, 70% of the subjects complained of some “other type of seat problems”. In extreme cases, female cyclists have experienced permanent swelling of the Labium Major caused by skin infections and lymphatic injury from the saddle. This conditioned has even been named “Bicyclist’s Vulva”. [6]
In 2003, a group of researchers released a series of bicycle related study findings in the Bicycle Saddle Report. Among these reports was a study that focused specifically on women titled, Ergonomics of 2 Bicycle Saddles. The study looked at 12 female subjects who rode on two different saddles for 30 minutes (Selle Royalgel with a flat gel top surface and the Selle Italia Ldy Trans Am with a hole cutout used as the control). The subjects rode in 40 degree and 60 degree positions and both pressure and comfort data were recorded. [7]

The results suggested that the mean pressure values between the two saddles were very similar (248 g/cm2 vs 267 g/cm2 for the RoyalGel and Ldy Trans Am, respectively). The main significant difference was the amount of contact surface area between the saddles. The RoyalGel saddle displayed 10 cm2 and 11 cm2 more contact surface area than the Ldy Trans Am in the in 40 degree and 60 degree positions, respectively. This increased surface area aided in dispersing the contact pressure of the rider and resulted in greater reports of comfort on the RoyalGel saddle.
By visually inspecting the pressure maps, it is clear that the pressure is spread more evenly over the RoyalGel saddle. In contrast, the Ldy Trans Am displays higher pressure readings at the edges of the hole.
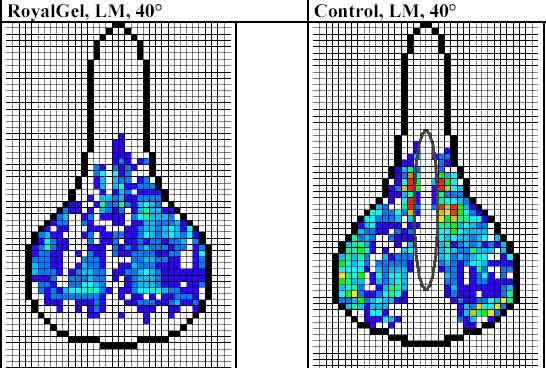
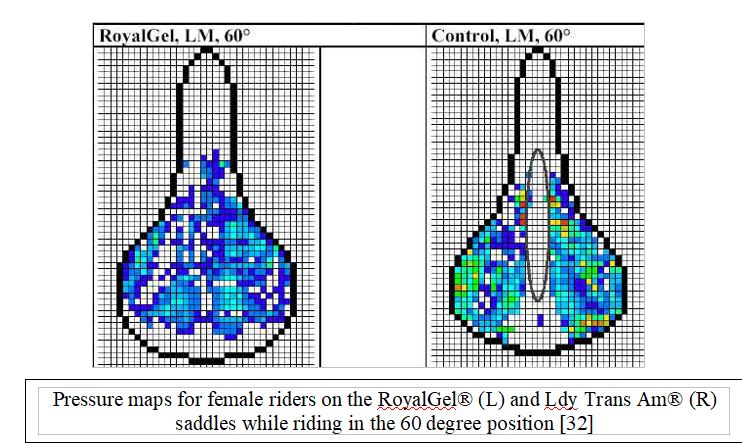
The authors concluded that female cyclists should avoid riding on saddles with holes due to the decreased contact surface and high pressures around the borders of the hole that may increase the risk of impairing blood flow and lymphatic drainage to a woman’s genitalia. It is also possible that the Labium Major can get compressed into the cutout region and result in increased compression of the nerves and arteries that supply the genitals. [7]
In Review
After close inspection of the differences between the two sexes in relation to the bicycle seat, the primary differences are the location of the external genitalia and the female’s increased infrapubic angle. The actual distance between a woman’s sit bones depends on that individual’s skeletal dimensions and may not always be larger than a male’s. As any rider leans further forward, the sit bones become less of a weight-bearing structure and the top curvature of the saddle becomes more important to avoid upward compression into the perineal region. There is strong evidence that saddles marketed to women with holes cutout of the support surface may not be beneficial. These holes may increase tissue injury as well as increasing compression of surrounding lymphatic, neural, and vascular structures. Although concerns about erectile dysfunction due to arterial and nerve compression while riding are often pushed aside as a male only concern, women should also be aware of the impact that saddles can have on these pelvic structures. Compression and injury to these same arteries and nerves in women can negatively impact the function of the clitoris and external genitalia and result in similar sexual dysfunctions.
Male Anatomy
Discussion of bicycle seat related problems often turns to whether or not a bicycle seat can cause erectile dysfunction. Many men consider this one of the more severe side effects of riding and wish to avoid such ailments at any cost. Some riders have reported being so disgruntled by the media’s reports of erectile dysfunction from bicycle seats that they removed their seats and posts altogether and began standing for entire rides. In light of all this concern, it is useful to understand how the anatomy functions to achieve an erection in order to determine if a bicycle seat can truly cause this problem.
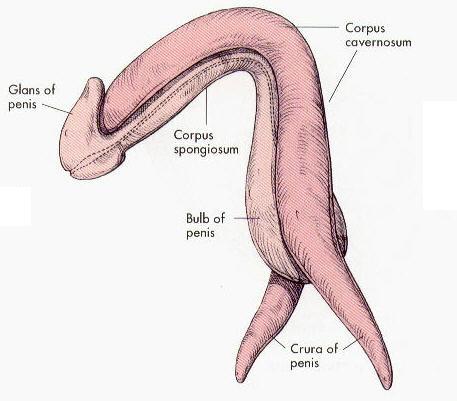
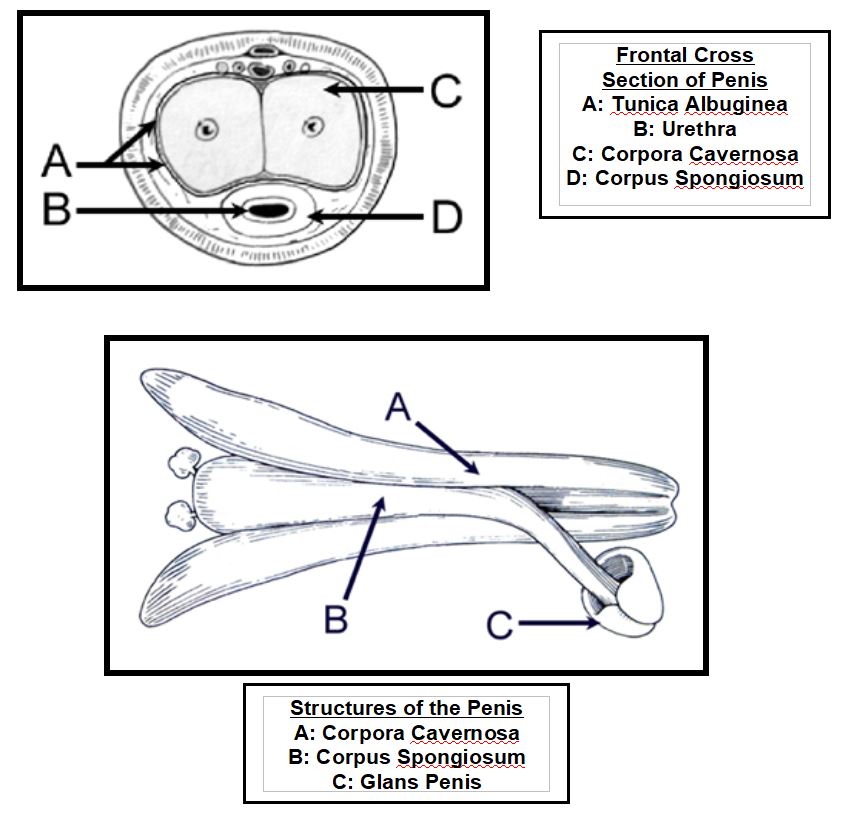
Complete erection of the penis is caused by a complex series of interactions between the nerves, arteries, and the veins. Within the shaft of the penis is a set of erection chambers (corpora cavernosa). These structures are composed of spongy tissues that are able to swell and expand when filled with blood.[8] Although it may seem a bit coarse, the structure of the penis can be compared to a hot dog in a bun, wrapped in paper. The erection chambers, or the two parts of the bun, are designed to engorge with blood when arteries that supply them are signaled to expand. These are the primary erectile structures for the penis. When the erectile chambers expand, they press against the paper wrapping (tunica albuginea) which results in a rigid erection. The hot dog section (corpus spongiosum), surrounds the urethra (the long tube that allows urine and semen to be discharged through the penis). At the end of the hot dog section is the glans penis, which is the highly sensitive cap on the very end of the penis.
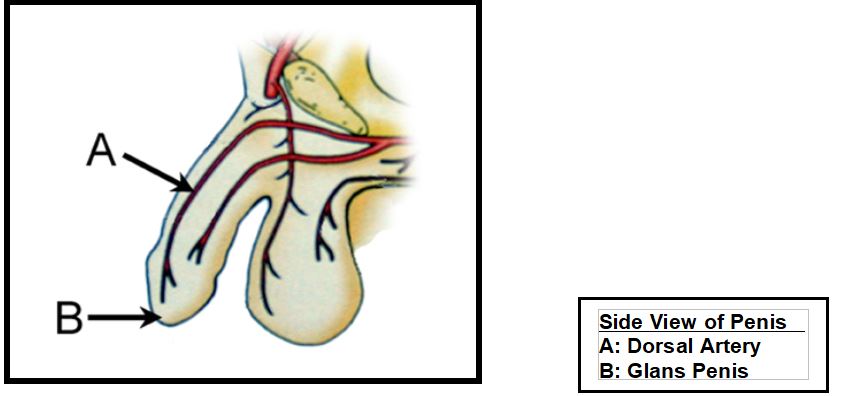
Arteries are vessels that allow blood to travel from the heart to other parts of the body. The dorsal penile artery is the primary blood supply for the penile structures. This artery is the terminal branch of the internal pudendal artery, which originates from deeper arteries within the pelvis. The internal pudendal artery courses along the inner aspect of the pubic rami (a bony portion of the pelvis), along with the pudendal nerve, all within a sheath termed Alcock’s canal.
When the penis is flaccid or limp, there is a permanent contraction of the smooth muscle surrounding the arteries. This contraction around the artery acts as a valve to limit the entry of blood into the spongy, erectile chambers of the penis. The smooth muscle that surrounds the arteries is activated to constrict by excitatory (i.e. sympathetic) nerve fibers. This means that when your body is reacting to physiological or psychological stress, the nervous system actually inhibits the penis from becoming erect by closing the valves on the vessels that carry blood to the penis.
During initiation of erection, the smooth muscle relaxes and allows blood flow into the erectile structures. As the spongy, erectile tissues expand, they press against a fibrous sheath (tunica albuginea) that limits further engorgement and swelling. The increased pressure within the sheath compresses the veins that allow the blood to flow out of the penis and back to the heart. This decrease of blood out of the penis results in increased penile rigidity and erection. The pudendal nerve is responsible for contraction of the penile musculature during ejaculation, transmitting sensation from the penis, and creating maximum penile rigidity.[8]
In Review
The anatomical structures and physiological events involved in creating and maintaining an erection can be quite complex. Very basically, the process can be broken down into four steps.
-
The nervous system has to trigger increased blood flow to the penis.
-
Blood has to be able to flow into the penis.
-
The tissue in the penis has to expand when the blood enters.
-
Return of blood out of the penis has to be decreased to increase penile rigidity.
If any of these steps are compromised due to nerve damage, artery or vein damage, or changes in the structure of the erectile tissues, erectile dysfunction may result.
References
1. McGurn, J., On Your Bicycle: An Illustrated History of Cycling. 1987, New York: Facts On File Publications. 207.
2. Dodge, P., The Bicycle, ed. S. Steedman. 1996, Paris: Flammarion.
3. Hippocrates, Airs Water Places. In Hippocrates. Vol. 1. 1923, London: William Heinemann. 125-31.
4. Sauer, J.P., J. Weisshaar, C. et al., Influence of Gender, Power, and Hand Position on Pelvic Motion during Seated Cycling. Medicine and Science in Sports and Exercise, 2007. 96(12): p. 2204-2211.
5. Bressel, E.C., J, Bicycle Seat Interface Pressure: Reliability, validity, and Influence of Hand Position and Workload. Journal of Biomechanics, 2005. 38(6): p. 1325-1331.
6. Baeyens, L.V., E. Bourgeois, P., Bicyclist's Vulva: observational study. BMJ, 2002. 325: p. 138-9 (20 July).
7. Frobose, I.B., L. et al., Ergonomics of 2 Bicycle Saddles: Pressure at the Pudendal Area in Women of a Normal Saddle with Gel and of a Saddle with a Hole. 2003 Bicycle Saddle Report / Projekt Wellcom, 2003: p. 1-15.
8. Clemente, C.D., Clemente Anatomy. 4 ed. A regional Atlas of the Human Body, ed. J. Velker. 1997, Baltimore: Williams and Wilkins.
9. Vuong, P., Peri Nodular Indurations ("Accessory Testicals") in Cyclists. ACTA Cytologica, 1988. 32: p. 86-90.
10. Mellion, M.B., Common cycling injuries. Management and prevention. Sports Med, 1991. 11(1): p. 52-70.
11. Weiss, B.D., Clinical syndromes associated with bicycle seats. Clin Sports Med, 1994. 13(1): p. 175-86.
12. Andersen, K.V. and G. Bovim, Impotence and nerve entrapment in long distance amateur cyclists. Acta Neurol Scand, 1997. 95(4): p. 233-40.
13. Huang, V.M., R. Goldstein, I., Bicycle Riding and Erectile Dysfunction: An Increase in Interest. Journal of Sexual Medicine, 2005. 2(5): p. 596-604.
14. Asplund, C.B., T. Weiss, B., Genitourinary Problems in Bicyclists. Current Sports Medicine Reports, 2007. 6(5): p. 333-339.
15. Dettori, J.K., TD. Cummings, P. Corman, JM., Erectile dysfunction after a long-distance cycling event: associations with bicycle characteristics. Journal of Urology, 2004. 2(172): p. 637-41.
16. Schrader, S.B., M. Lowe, B., Health and Hazard Evaluation Re-port. Long Beach, California. National Institute for Occupational Safety and Health, 2001. 5.
17. Nehra, A., et al., Mechanisms of venous leakage: a prospective clinicopathological correlation of corporeal function and structure. J Urol, 1996. 156(4): p. 1320-9.
18. Schrader, S.B., BS. Lowe, B., Cutting off the Nose to Save the Penis. Journal of Sexual Medicine, 2008. e-journal article In Press.
19. Kyle, C.R., The Mechanics and Aerodynamics of Cycling. Medical and Scientific Aspects of Cycling. 1988, Champaign, IL: Burke Er and Newsom MM.
20. Schwarzer, U., Impotence Rate in Long Distance Cyclists. Journal of Urology, 1999. 161: p. 686A.
21. Solomon, S. and K.G. Cappa, Impotence and bicycling. A seldom-reported connection. Postgrad Med, 1987. 81(1): p. 99-100, 102.
22. Pisco, J.M., et al., Changes in the vasa vasorum following percutaneous transluminal angioplasty in a canine model of aortic stenosis. J Vasc Interv Radiol, 1994. 5(4): p. 561-6.
23. Pisco, J.M., et al., Vasa vasorum changes following stent placement in experimental arterial stenoses. J Vasc Interv Radiol, 1993. 4(2): p. 269-73.
24. Maurice, G., X. Wang, and J.F. Stoltz, Linear and nonlinear elastic modelling of the deformation of vasa vasorum. Clin Hemorheol Microcirc, 1998. 19(4): p. 291-8.
25. Maurice, G., et al., [Modeling of elastic deformation and vascular resistance of arterial and venous vasa vasorum]. Journal des Maladies Vasculaires, 1998 Oct. 23(4): p. 282-8.
26. Oberpenning, F., et al., The Alcock syndrome: temporary penile insensitivity due to compression of the pudendal nerve within the Alcock canal. J Urol, 1994. 151(2): p. 423-5.
27. Specialized, I., www.specializedbikes.com/Medical Studies, . 2001.
28. Kerstein, M.D., et al., Perineal trauma and vasculogenic impotence. J Urol, 1982. 127(1): p. 57.
29. Bader, D.L., The recovery characteristics of soft tissues following repeated loading. J Rehabil Res Dev, 1990. 27(2): p. 141-50.
30. Henderson, J., Efficacy of three measures to relieve pressure in seated persons with spinal cord injury. Arch Phys Rehabil, 1994. 75(May): p. 535-539.
31. Bar, C.A., Evaluation of cushions using dynamic pressure measurement. Prothetics and Orthotics International, 1991. 15: p. 232-240.
32. Rodano, R.S., R. Sacchi, M. et al. Pressure Distribution on Bicycle Saddles. in Symposium of the International Society of Biomechanics in Sports. 2002: ISBS.
33. Lowe, B.S., S. Breitenstein, M., Effects of Bicycle Saddle Designs on the Pressure to the Perineum of the Bicyclist. Medicine and Science in Sports and Exercise, 2004. 36(6): p. 1055-1062.
34. Wilson, H. and S. Hutchinson, Understanding and Evaluating Nursing Research, in Consumer's Guide to Nursing Research. 1996, Delmare Publishers: New York. p. 155-158.
35. Borgia, J.F. and S.M. Horvath, Transcutaneous, noninvasive PO2 monitoring in adults during exercise and hypoxemia. Pflugers Arch, 1978. 377(2): p. 143-5.
36. McDowell, J.W. and W.H. Thiede, Usefulness of the transcutaneous Po2 monitor during exercise testing in adults. Chest, 1980. 78(6): p. 853-5.
37. Kessler, R., Personal communication regarding seat experimentation, . 2000, Professor of Urology, Stanford University.
38. Nayal, W., et al., Transcutaneous penile oxygen pressure during bicycling. BJU Int, 1999. 83(6): p. 623-5.
39. Sommer, F., et al., [Changes in penile blood flow during cycling--how does one prevent a decreased perfusion?]. Dtsch Med Wochenschr, 2001. 126(34-35): p. 939-43.
40. Bressel, E.R., T. Parker, D. et al., Influence of Bicycle Seat Pressure on Compression of the Perineum: a MRI analysis. Journal of Biomechanics, 2007. 40: p. 198-202.
41. Cohen, J., Gross, M., Effect of bicycle racing saddle design on transcutaneous penile oxygen pressure. Journal of Sports Medicine and Physical Fitness, 2005. 45(3): p. 409-18.
42. Sommer, F., et al., Impotence and genital numbness in cyclists. Int J Sports Med, 2001. 22(6): p. 410-3.
43. Gemery, J.N., A. Mamourian, A. et al., Digital Three-Dimensional Modelling of the Male Pelvis and Bicycle Seats: Impact of Rider Position and Seat Design on Potential Penile Hypoxia and Erectile Dysfunction. BJU Int., 2007. 99(1): p. 135-40.
44. Nordeen-Snyder, K.S., The effect of bicycle seat height variation upon oxygen consumption and lower limb kinematics. Med Sci Sports, 1977. 9(2): p. 113-7.
45. Website, A.S., Allay Saddles -- The Latest Research, . 2008, http://www.allaysaddles.com/research/research.htm.